IDSA 2025 Guideline Update on Complicated Urinary Tract Infections
Introduction
The prior version of the IDSA UTI guidelines focused on uncomplicated cystitis and pyelonephritis in women, omitting complicated UTI (cUTI) and UTI in men. Since the publication of those guidelines, many randomized, controlled trials assessing new antimicrobials for cUTI in both women and men have been published. Women have a lifetime risk of 53% of experiencing UTI. While UTI is uncommon in men prior to age 50, their lifetime risk is a nontrivial 14%. Risk of experiencing a UTI increases with age in both sexes. Given the aging US population, UTI in men is a salient issue, as is UTI in women. Fortunately, a reasonable evidence base now exists to support guidelines for treatment of cUTI in men and women.
Gram-negative urinary organisms collected from outpatients across all regions of the United States now have antimicrobial resistance rates above the thresholds recommended for using antibiotics as empiric treatment of UTI in the 2010 guidelines. In the face of these concerningly high rates of resistance, the evidence needed to guide empiric choice of antibiotics for treating UTIs needs to be reevaluated.
Classifications
These classifications are endorsed by AMMI-CA, ASM, AUA, ESCMID, SAEM, SHM, and SIDP
Section last reviewed on 05/12/2025
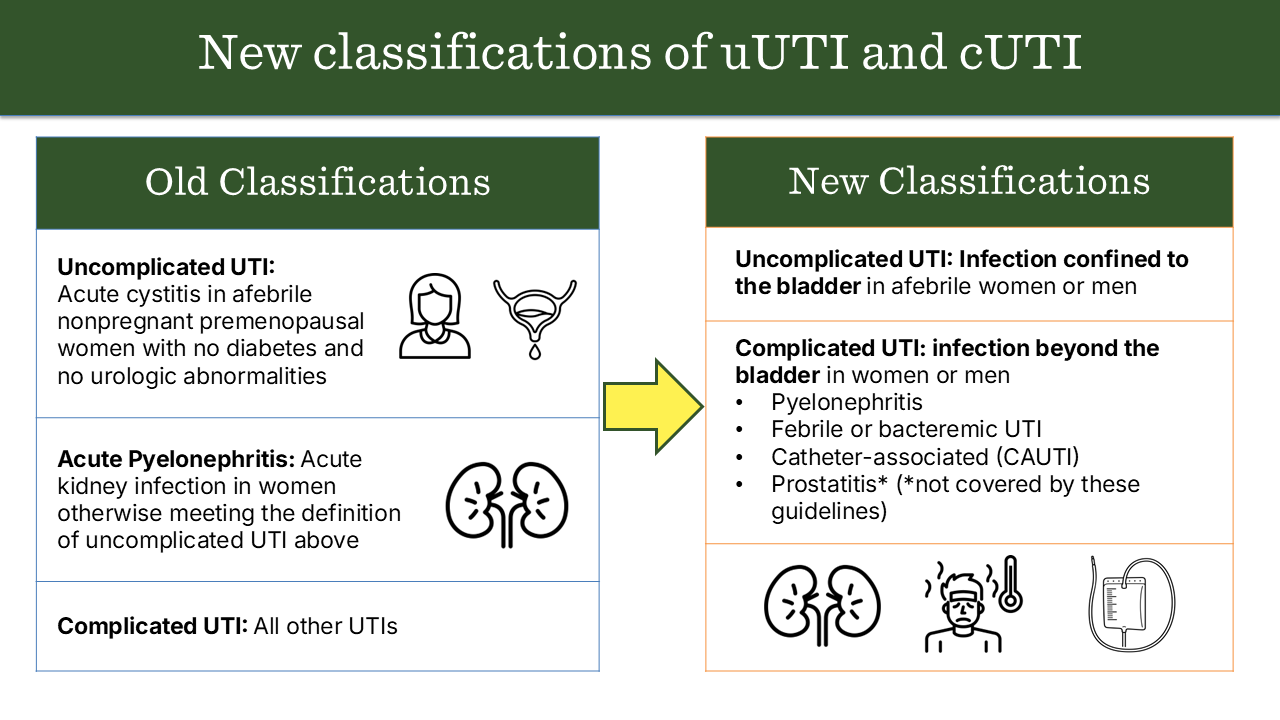
We perceived a need to update the classifications of uncomplicated and complicated UTI to better align with clinical practice, become more congruent with the available data on male UTI, and better guide management decisions. We therefore focused our revised classifications of uncomplicated and complicated UTI on the presence or absence of localized or systemic symptoms, particularly fever, that would suggest the infection had progressed beyond the bladder. We also focused the revised classifications on factors that would be readily apparent to the treating clinician at the point of care (e.g., vital signs and catheterization) rather than factors that might not be apparent without a urologic evaluation (e.g., anatomic abnormalities or urinary retention). Please refer to the full manuscript for nuances of the classifications.
Figure 1.0: Comparing prior and updated classifications of uncomplicated and complicated UTI
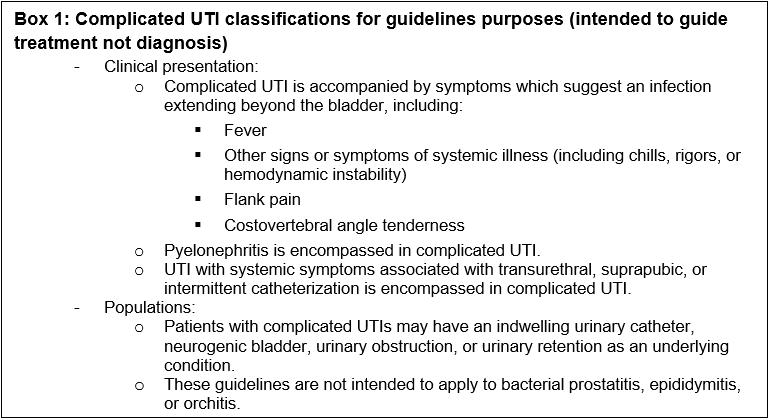
Box 1: Complicated UTI classifications for guidelines purposes (intended to guide treatment not diagnosis)
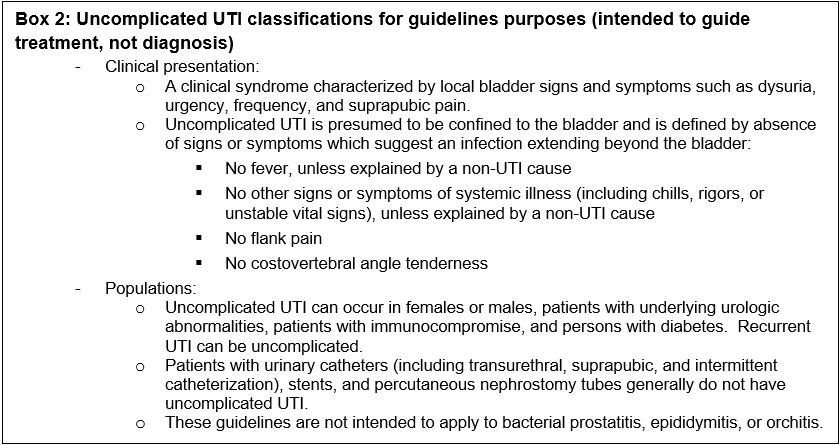
Box 2: Uncomplicated UTI classifications for guidelines purposes (intended to guide treatment, not diagnosis)
Methods
The panel included physicians and pharmacist with expertise in infectious diseases, medical microbiology, hospital medicine, primary care, emergency medicine, gynecology-obstetrics, urology, and pharmacology. The following organizations reviewed and provided feedback on the associated manuscripts: SIDP (Society of Infectious Diseases Pharmacists), AAFP (American Academy of Family Physicians), SHM (Society of Hospital Medicine), AUA (American Urological Association), ASM (American Society of Microbiology), SAEM (Society for Academic Emergency Medicine), AMMI-CA (Association of Medical Microbiology and the Infectious Disease Canada), European Society of Clinical Microbiology and Infectious Diseases (ESCMID).
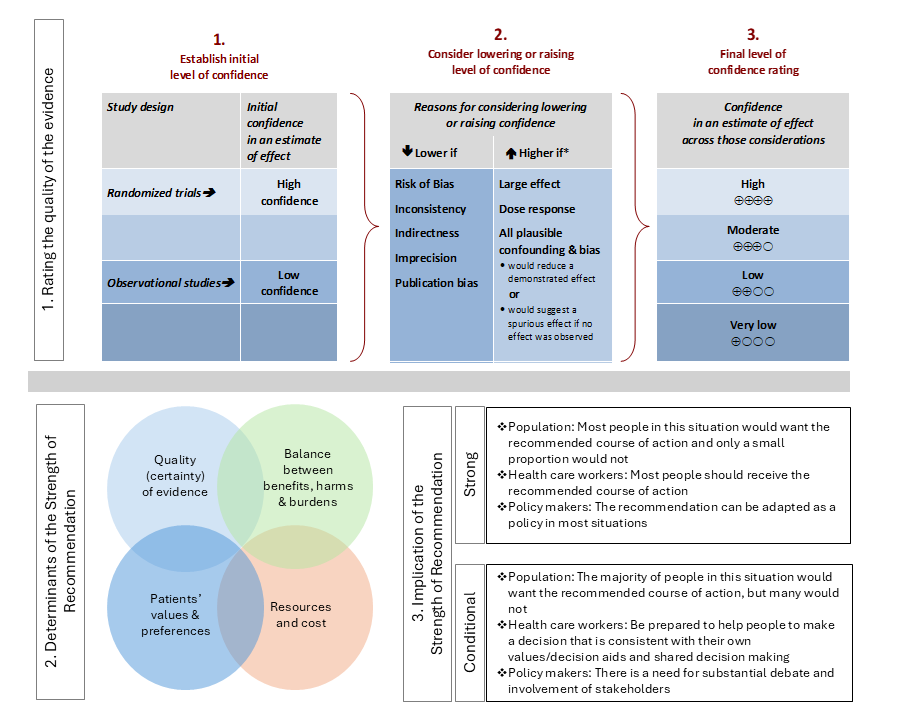
For each question, a systematic review was performed to identify relevant studies, and the GRADE (Grading of Recommendations Assessment, Development, and Evaluation) approach was followed for assessing the certainty of evidence and strength of recommendation (Figure 2.0).
Details of the systematic review and guideline development processes are available in the supplemental materials for each included manuscript.
Figure 2.0. Approach and implications to rating the quality of evidence and strength of recommendations using GRADE methodology (unrestricted use of figure granted by the U.S. GRADE Network)
Recommendations on the Selection of Antibiotic Therapy for Complicated UTI
These recommendations are endorsed by AMMI-CA, ASM, AUA, ESCMID, SAEM, SHM, and SIDP
Section last reviewed on 05/12/2025
Last literature search conducted September 2024
[View supplemental material here]
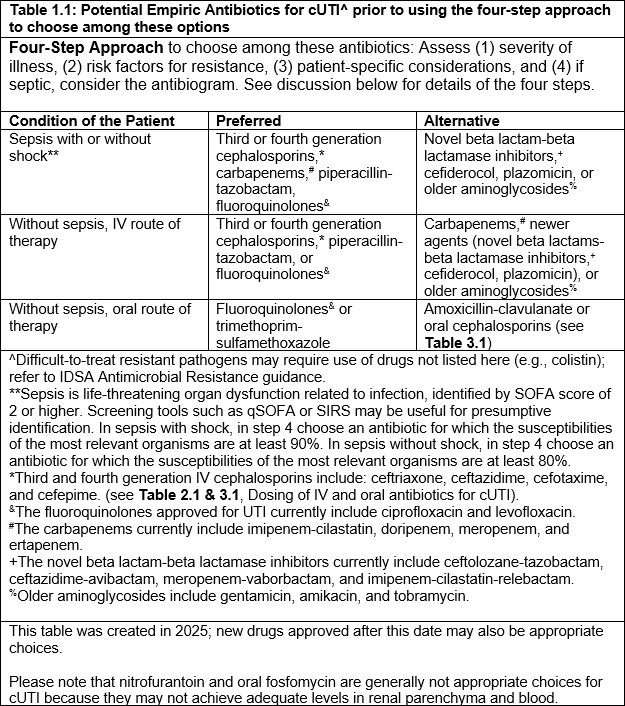
The scope of this clinical question is the empiric choice of antibiotics in suspected cUTI. The guidelines categorize empiric antibiotic choices as preferred versus alternative, stratified for severity of illness. However, when choosing among these antibiotics for a specific patient, a four-step process should be followed to account for changing resistance patterns and individualized patient needs. Specifically, the four-step approach is to assess: (1) severity of illness, (2) risk factors for resistance, (3) patient-specific considerations, and (4) if septic, consider the antibiogram.
A. Initial Selection Among Empiric Antibiotic Options for Complicated UTI
In patients with cUTI, which classes of empiric antibiotic therapy should initially be prioritized?
Recommendations
a) For patients with sepsis due to complicated UTI, we suggest initially selecting among the following antibiotics, using the four-step assessment (Figure 1.1): third- or fourth-generation cephalosporins, carbapenems, piperacillin-tazobactam, or fluoroquinolones, rather than newer agents or older aminoglycosides (conditional recommendation, very low to moderate certainty of evidence).
Remarks
- See Table 1.1 for a more complete list of empiric antibiotic therapy options.
- Please refer to the four-step approach in Figure 1.1 to choose among these antibiotics for the specific patient.
- Agents with broader spectrum of activity against organisms other than Enterobacterales (e.g. Pseudomonas aeruginosa, enterococci, or methicillin-resistant Staphylococcus aureus) may be considered for patients with sepsis in whom the diagnosis of cUTI is not clear or who are suspected to have cUTI due to these pathogens.
Comments
- This recommendation places a higher value on providing early, appropriate empiric antibiotic therapy to prevent mortality while deferring stewardship considerations to definitive therapy.
- The certainty of evidence was moderate for all classes of antibiotics, except for third and fourth generation cephalosporins, and older aminoglycosides, for which the certainty of evidence was very low.
b) For patients with suspected complicated UTI without sepsis, we suggest initially selecting among the following antibiotics, using the four-step assessment (Figure 1.1): third- or fourth-generation cephalosporins, piperacillin-tazobactam, or fluoroquinolones, rather than carbapenems and newer agents or older aminoglycosides (conditional recommendation, very low to moderate certainty of evidence).
Remarks
- See Table 1.1 for a more complete list.
- Refer to the four-step approach in Figure 1.1 to choose among these antibiotics for the specific patient.
- Other agents (e.g., trimethoprim-sulfamethoxazole, amoxicillin-clavulanate, first or second-generation cephalosporins) are less well studied but may be appropriate in select settings for empiric oral treatment of cUTI.
Comments
- This recommendation places a higher value on antibiotic stewardship in patients with cUTI who are not septic while also considering costs, resources, and practical aspects of antibiotic administration.
- The certainty of evidence was moderate for all classes of antibiotics, except for third and fourth generation cephalosporins and older aminoglycosides, for which the certainty was very low.
Table 1.1: Potential Empiric Antibiotics for CUTI
B. Process to Guide Empiric Antibiotic Choice for Complicated UTI
To optimize the selection of empiric antibiotic therapy for patients with suspected complicated UTI, we propose the following four-step approach: 1) assess the severity of illness, 2) consider patient-specific risk factors for resistant uropathogens, 3) evaluate other patient-specific considerations, and 4) for patients with sepsis, consult a relevant local antibiogram if available.
Figure 1.1: Four-step approach to choosing empiric antimicrobial therapy for cUTI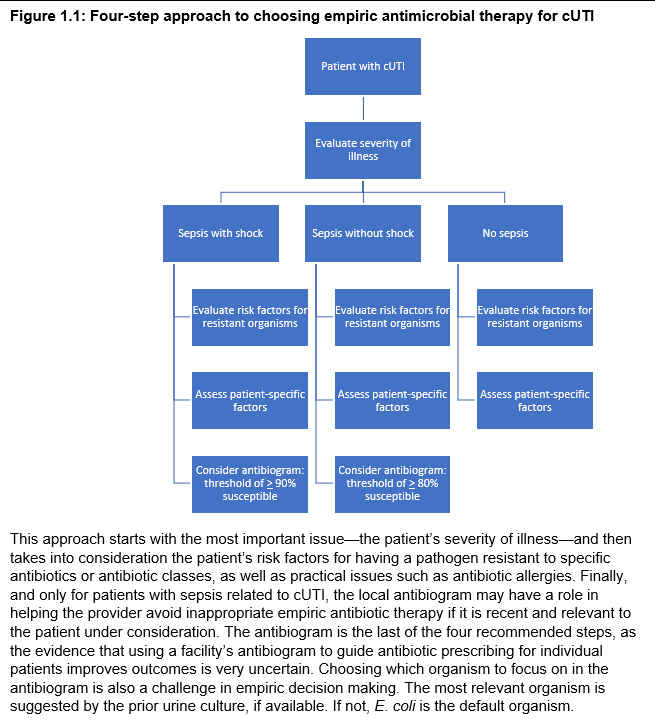
STEP 1: SEVERITY OF ILLNESS
In patients with suspected cUTI (including pyelonephritis), should selection of empiric antibiotic therapy be guided by severity of illness?
Recommendation
I. For patients with suspected complicated UTI, we suggest that selection of empiric antibiotic therapy be initially guided by whether the patient is in sepsis or not (conditional recommendation, very low certainty of evidence).
Remarks
- Sepsis is defined per the Sepsis-3 Task Force as life-threatening organ dysfunction caused by a dysregulated host response to infection. Patients can be identified by SOFA score increase of 2 points or more or with screening tools such as qSOFA or SIRS.
STEP 2: PATIENT-SPECIFIC RISK FACTORS FOR RESISTANT UROPATHOGENS
Should empiric antibiotic therapy be guided by prior urine cultures and risk factors for resistant uropathogens?
Recommendations
I. In patients with complicated UTI, we suggest avoiding antibiotics to which the patient previously had a resistant pathogen isolated from the urine (conditional recommendation, very low certainty of evidence).
Remarks
- More recent urine cultures may be a better guide than more distant urine cultures. The median time frame for paired cultures was 3-6 months.
II. In patients with complicated UTI, we suggest avoiding fluoroquinolones if the patient has been exposed to that class in the past 12 months (conditional recommendation, very low certainty of evidence).
Remark
- More recent antibiotic exposure may be a better guide than more distant exposure.
STEP 3: OTHER PATIENT-SPECIFIC CONSIDERATIONS
Should empiric antibiotic therapy selection account for patient-specific considerations?
Recommendation
I. In suspected cUTI, empiric antibiotic therapy selection should account for risk of allergy, contraindications, or drug interactions to avoid preventable adverse events (good practice statement).
STEP 4: ANTIBIOGRAM
Should empiric antibiotic therapy be further tailored by consulting an antibiogram?
Recommendations
I. In patients with sepsis assumed to be caused by complicated UTI, we suggest using a local, recent, and relevant antibiogram to further tailor empiric antibiotic choice (conditional recommendation, very low certainty of evidence).
Remarks
- An antibiogram is local if derived from the same facility, recent if based on data from the prior 12 months, and relevant if based on similar organisms.
- Consider selecting an antibiotic for which ≥90% of the most relevant organism(s) are susceptible in patients in septic shock, or ≥80% in sepsis without shock.
- Septic shock is defined by need for vasopressors despite volume resuscitation and serum lactate >2 mmol/L.
II. For patients with suspected complicated UTI without sepsis, we make no specific recommendation on using an antibiogram (no recommendation, knowledge gap).
Remarks
- Routine use of broader-spectrum agents in suspected complicated UTI without sepsis may drive resistance.
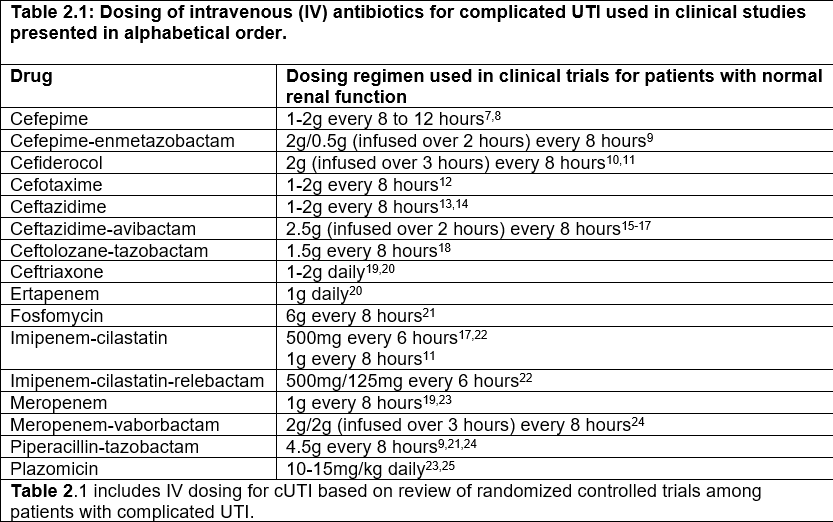
Table 2.1: Dosing of intravenous antibiotics for complicated UTI
C. Selection of Definitive Antibiotic Therapy for Complicated UTI
Should definitive therapy be targeted based on urine culture?
Recommendation
I. In confirmed complicated UTI, we suggest selecting a definitive effective antibiotic with a targeted spectrum based on urine culture (identification and susceptibility) as soon as available, rather than continuing empiric broad-spectrum antibiotics for the full duration (conditional recommendation, low certainty).
Comment
- This places a high value on de-escalating therapy based on culture, optimizing effectiveness, and stewardship. De-escalation may be less practical in outpatient cUTI.
References: View full reference list here
Recommendations on the Timing of Intravenous to Oral Antibiotics Transition for Complicated UTI
These recommendations are endorsed by AMMI-CA, ASM, AUA, ESCMID, SAEM, SHM, and SIDP
Section last reviewed on 05/12/2025
Last literature search conducted September 2024
[View supplemental material here]
An increasing number of clinical trials support early IV treatment with transition to oral therapy for infectious syndromes. From a pharmacological point of view, antibiotic efficacy depends on the levels of the antibiotic obtained in serum and tissue, not the route of administration. In practice, providers often switch from intravenous to oral antibiotics during cUTI therapy, once a patient is clinically improving. We sought evidence about whether this transition impacts clinical outcomes versus continued intravenous therapy, and about optimal timing for switch.
From a practical perspective, an IV to oral switch, if equivalent in outcomes, is desirable because it can reduce the need for intravenous access, complications, nursing time, medication volume, hospital stay, costs, and inconvenience.
Some patients with cUTI can be managed entirely with oral antibiotics in the outpatient setting. See also Table 1.2.
In patients being treated parenterally for cUTI, who are clinically improving, able to take oral medication, and for whom an oral option is available, should parenteral therapy be transitioned to oral?
Recommendations
I. In cUTI (including acute pyelonephritis), treated initially with parenteral therapy and clinically improving, we suggest transitioning to oral antibiotics rather than continuing parenteral therapy (conditional recommendation, low certainty of the evidence).
Comments
- This recommendation values reducing intravenous catheter-related adverse events, costs, and practical administration aspects.
- Studies excluded patients with indwelling catheters, sepsis, immunocompromised states, severe renal insufficiency, and functional/structural urinary tract abnormalities. Some subpopulations may need individualized therapy.
- An effective agent achieves therapeutic urine/tissue levels and is active against the pathogen.
- See Figure 1.2 for stepwise approach.
II. In cUTI with Gram-negative bacteremia, treated with parenteral antibiotics, and clinically improving, we suggest transition to oral antibiotics if possible (conditional recommendation, very low certainty).
Comments
- Most trials included afebrile, hemodynamically stable patients who achieved source control before oral switch.
- Effective oral agent for bacteremia must achieve therapeutic blood, urine, and tissue levels.
- See Figure 1.2 for stepwise assessment.
Figure 1.2: Stepwise assessment of IV to oral switch and antibiotic duration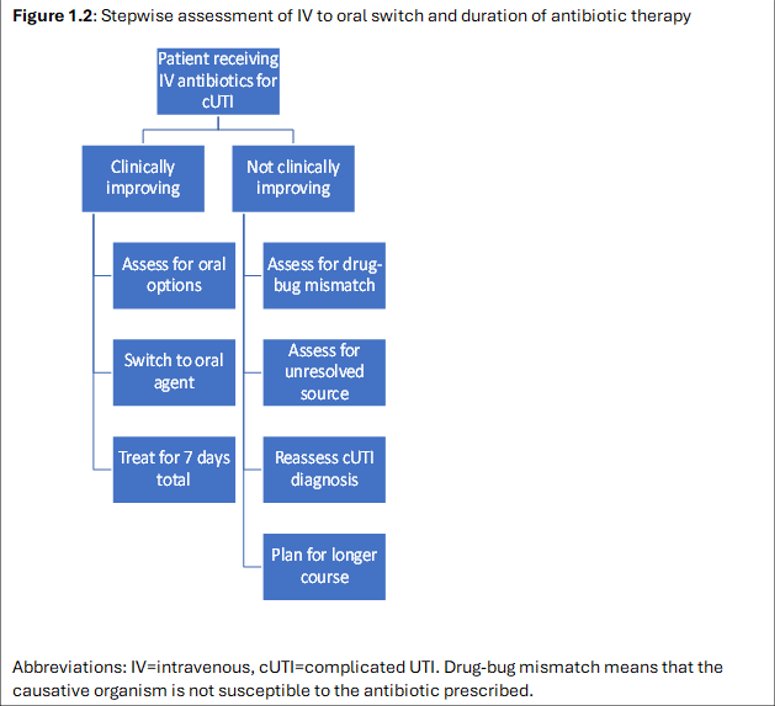
Table 1.2: Dosing of oral antibiotics for complicated UTI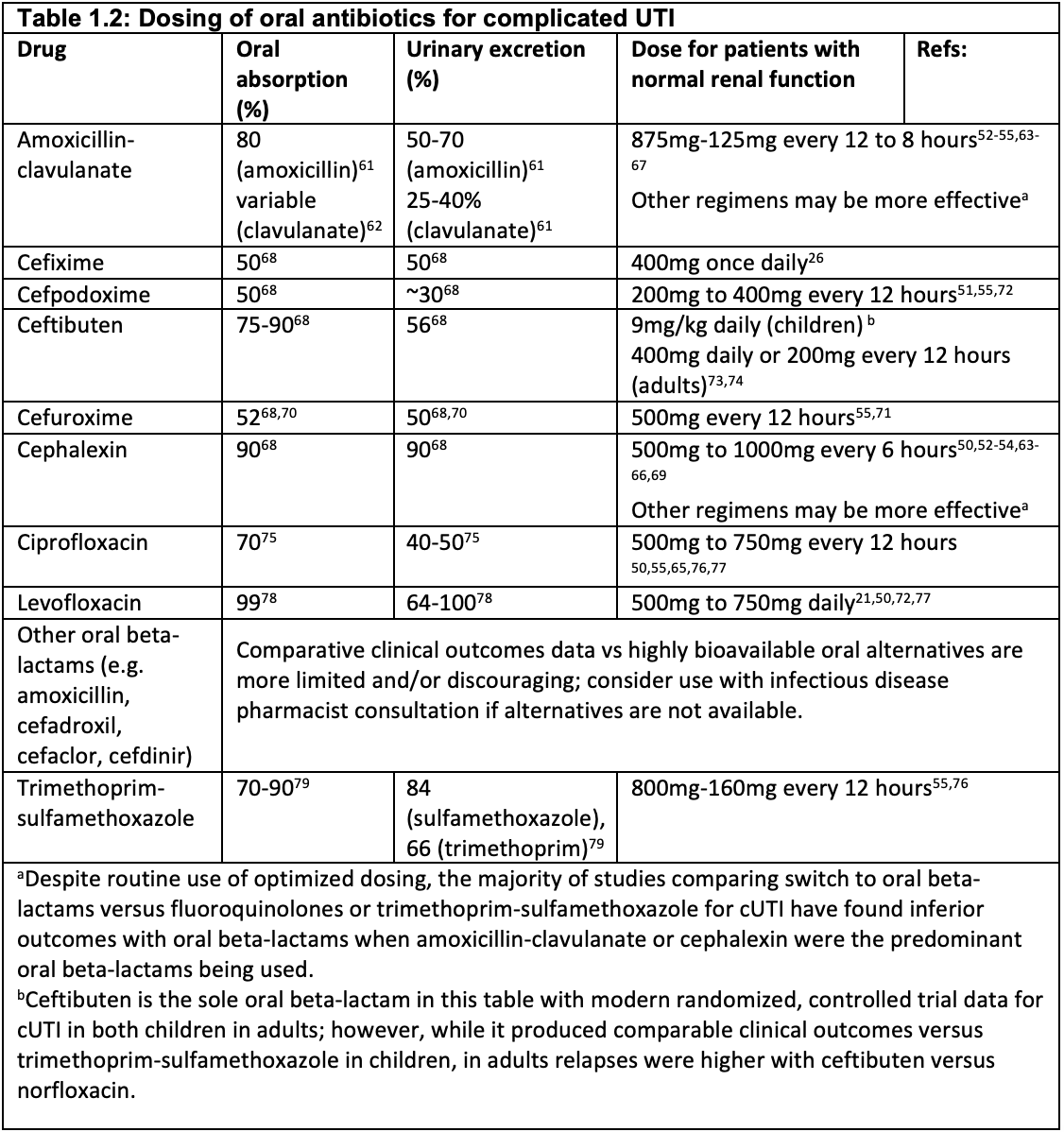
References: View full reference list here
Recommendations on the Duration of Antibiotics for Complicated UTI
This recommendation is endorsed by AMMI-CA, ASM, AUA, ESCMID, SAEM, SHM, and SIDP
Section last reviewed on 03/12/2025
Last literature search conducted September 2024
[View supplemental material here]
The duration of therapy is important for antibiotic stewardship and patient wellbeing. Many studies show that infections are often treated for longer than needed, and excess antibiotic exposure increases risk of adverse effects and antimicrobial resistance.
In patients with complicated UTI and clinical response to therapy, should duration be >7 days or shorter (≤7 days)?
Recommendations
I. In patients with complicated UTI (including pyelonephritis) who are improving clinically, we suggest a shorter course: 5–7 days of a fluoroquinolone or 7 days of a non-fluoroquinolone antibiotic (conditional recommendation, moderate/very low certainty of evidence), rather than 10–14 days.
Definitions
- An effective agent achieves therapeutic urine/tissue levels and is active against the causative pathogen. Duration is counted from the first day of effective therapy.
Comments
- Most trials excluded patients with indwelling catheters, severe sepsis, immunocompromise, abscesses, chronic kidney disease, bacterial prostatitis, complete obstruction, or urologic surgery. Some such patients may require individualized duration.
- Men with febrile UTI and possible acute prostatitis may benefit from longer treatment (10–14 days).
- This recommendation is based mainly on fluoroquinolone trials; less evidence exists for oral beta-lactams and higher doses may be needed for efficacy.
- Evaluate patients who do not improve promptly for ongoing sources of infection requiring intervention.
- This prioritizes stewardship and patient-centered reduction of therapy.
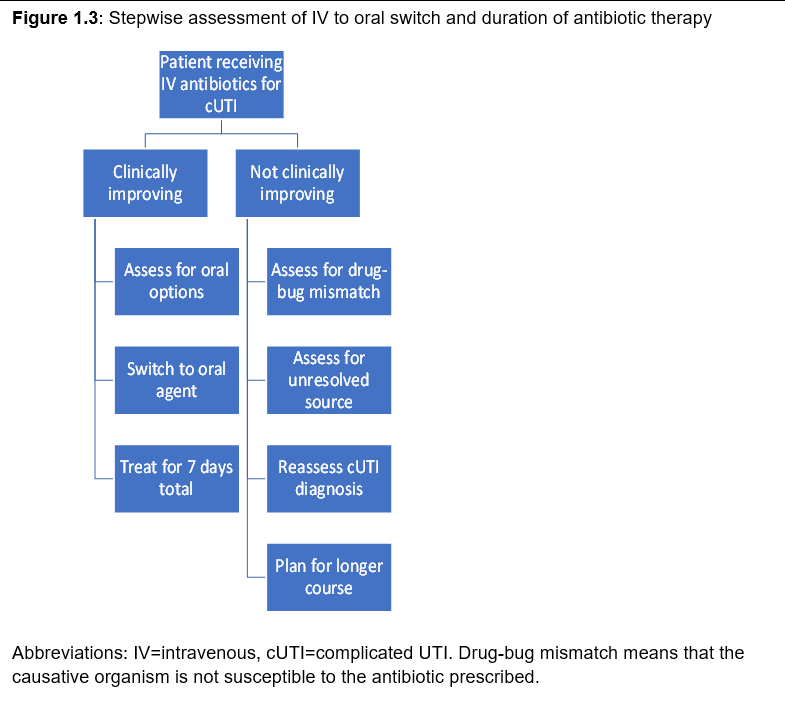
- See Figure 1.3 for a stepwise approach to switching and duration.
II. In complicated UTI with Gram-negative bacteremia who are clinically improving, we suggest 7 days of antimicrobial therapy rather than 14 days (conditional recommendation, low certainty).
Definitions
- For bacteremia, the agent must achieve therapeutic blood, urine, and tissue levels; duration is counted from the first day of effective therapy.
Comments
- Men with febrile, bacteremic UTI and possible prostatitis may benefit from longer duration.
- Evaluate for ongoing sources needing intervention if no prompt clinical improvement.
- See Figure 1.3 for stepwise assessment.
Figure 1.3: Stepwise assessment of IV to oral switch and duration
References: View full reference list here
Patient Perspectives
The evidence base for these guidelines is drawn from the general population of patients with cUTI who are healthy enough to enter clinical trials. Treatments are expected to relieve symptoms and prevent recurrence. However, a subset suffers from chronic urinary symptoms. Recommendations about chronic UTI or recurrent UTI are outside of the guideline's scope, but the panel acknowledges the importance of hearing patients' voices. Representatives from large patient advocacy groups participated in the patient advisory group; see the full manuscript for their detailed perspectives and research suggestions.
Notes
Acknowledgments
We acknowledge the important contributions of our four patient representatives (Carolyn Turner, Lisa Tecklenburg, Valerie Price, Laura Helgeson) and the two librarians (Elizabeth Kiscaden and Mary Beth McAteer). We appreciate the efforts of our three external reviewers and reviews by the Standards and Practice Guidelines Subcommittee. We also acknowledge IDSA staff for their support in guideline development.
Conflicts of Interest
Possible conflicts of interest. Evaluation of relationships as potential conflicts of interest is determined by a review process. Disclosed financial and professional relationships from panelists since 2019 are listed in full detail in the guideline. No disclosures were reported for all other authors.
Publication Disclaimer
© IDSA 2025. All rights reserved. No part of this publication may be reproduced, stored, transmitted, used for text and data mining, or training AI, in any form or by any means, without prior written permission or as expressly permitted by law. For commercial re-use, contact reprints@oup.com. All other permissions via Oxford University Press RightsLink. For further information, contact journals.permissions@oup.com.